My mission in life is not merely to survive, but to thrive; and to do so with some passion, some compassion, some humour, some style.
Category: Comunity First Responding
Posts relating to my role as a community first responded with East Midlands Ambulance Service (EMAS). All views are my own and do not represent the opinion of EMAS, or West Leicester CFR group. No patient specific information will be disclosed in any posts.
One job this evening, to an elderly patient who had fallen earlier in the afternoon hitting seemingly every limb on the way down.
The patient’s mid 50’s son dialled 911 for an ambulance (it’s 999 folks!) but still managed to summon help.
I was due to be meeting some CFR colleagues in the pub for a brainstorming session for our Soap Box derby (more on that in a later post perhaps!) and had all but sent my “OFD” (Off Duty) text message when I received the following call.
Resource Alloc. Call Details: {call number} **/03/2019 {Patient’s address}, Age **. Traumatic Injurys – Falls. Wrist is pointing the wrong way and hand and thigh deformed. Conscious-YES, Breathing-YES.
As well as cardiac arrests, we also get sent to trauma jobs but do not carry pain relief some CFRs are quite vocal in their opinions on this, in some cases I would agree but today I managed just fine without. Lucky on arrival ***** had been carried into bed by relatives and despite scoring 10/10 in pain was in good spirits.
After completing 2 full sets of observations I began writing up and completing the paperwork. It’s a pleasure to be able to spend the time with different people in the community, and this patient was a dream. I used the time not only to write an accurate history for the receiving Paramedics and Emergency Department, but to have a laugh with the patient. By the end of my time with them they said it still hurt just as bad as when I arrived but they felt much better in general.
So there you have it, a CFR can still help make a patient feel better even without pain relief!
Upon the arrival of the crew the good craic continued the the fantastic EMAS Paramedic and ECA until the patient was safely carried into the ambulance. Suspected neck of femur fracture, and broken wrist. Ouch!
Some excellent feedback from the crew: “I love it when we get paperwork as good as this – it makes our lives so much easier”
It’s been a while since I last wrote anything on here, mainly because life has been very hectic, but having stumbled across my own website, I thought I would share a story which, although sad, is quite fitting with my last post.
I have been a volunteer CFR for EMAS (East Midlands Ambulance Service) for over 3 years; I have volunteer 200 hours per year and attend on average 100 calls per year. Despite having received excellent training and being well prepared, I had never been allocated to a cardiac arrest.
That all changed in mid August 2018. I finished work at 5pm, and booked on as soon as I got home- opting to log on before making and eating dinner. However, no sooner had I sent the ‘On Duty’ text message, I received an immediate alert.
A call to help a patient who is not breathing is about one of the most serious calls we respond to, and this was my first as a solo responder. The piercing sound of my CFR Nokia’s “beep beep beep – beep beep – beep beep beep” made me jump straight into gear and into the car.
All CFRs must adhere to the rules of the road and we are not permitted to drive on blue lights. So despite having to stop at traffic lights and obey the speed limits I managed to arrive within 7 minutes of receiving the call.
Upon arrival at the patient’s address I was met by a relative who came out of the house to meet me. “****’s not responding” they said.
I quickly but calmly grabbed my kit bag and defibrillator, and made my way to the upstairs bedroom, checking for danger as I entered the house. Excellent CPR was being administered by a neighbour, recently trained in first aid at work. I checked the patient for a response. None. I checked that the airway was clear, which it was. For 10 very long, and very lonely seconds I looked, listened and felt for signs of breathing.
None.
Shit.
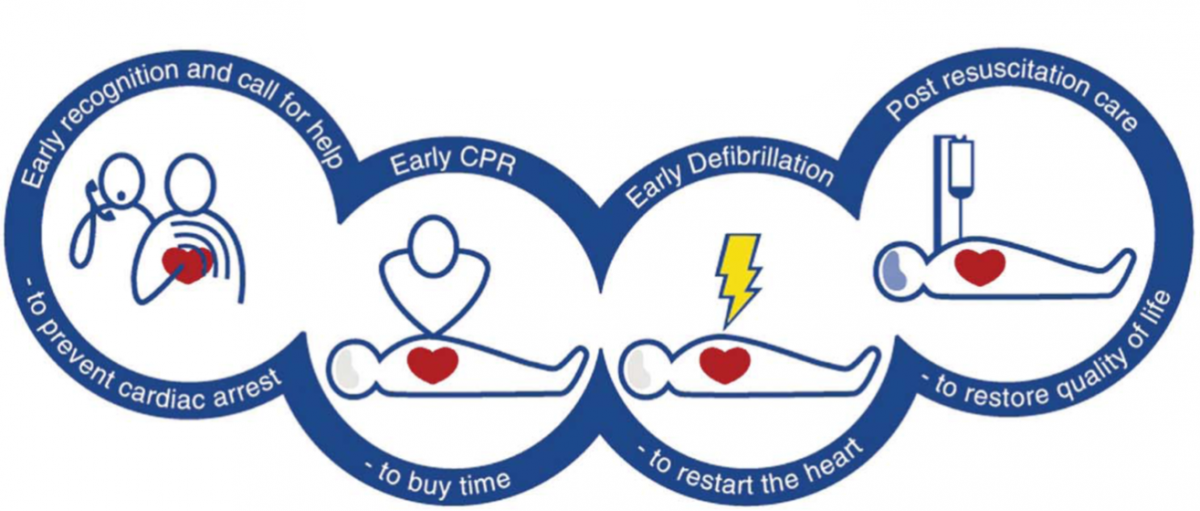
The neighbour recommenced CPR which allowed me to focus on getting the defibrillator pads on the patient’s bare chest, and phoning the CFR dispatch desk to confirm that this was a cardiac arrest. Many people aren’t aware that CPR alone will not ‘restart a heart’. CPR is one, very important link the chain of survival, its purpose being to get oxygen into a person’s lungs to prevent brain damage. In effect you buy time until a defibrillator arrives on scene. The importance of good and immediate CPR is reflected when you consider that in some cases, CPR can double the chances of survival from out of hospital cardiac arrest.(1)
The Chain of Survival
Whilst the defibrillator was analysing the patient’s heart rhythm, I took the time to measure and insert an OPA (Oropharyngeal airway) to ensure that through the resuscitation attempt the maximum amount of Oxygen was being administered to the patient.
Oropharyngeal Airway (OPA)
I then set up a BVM (Bag Valve Mask) with 15lpm of Oxygen, the defibrillator advised ‘No shock’ so I took over CPR, using a ratio of 30 chest compression to 2 rescue breaths using the BVM until the AED told me to stop in order for it to perform another analysis cycle.
Bag Valve Mask (BVM)
At this point, ****, an EMAS Paramedic from Hinckley ambulance station arrived on scene, and we worked together until the second ambulance crew arrived. Me doing chest compressions and the Paramedic establishing IV access and an advanced airway.
Upon the arrival of the ambulance the CFR’s role is to assist the Paramedic, and what happened next was a blur, with ROSC (Return of Spontaneous Circulation) achieved twice, but unfortunately not sustainable.
There is a fine line between helping and getting in the way, so I made a conscious effort to do things I knew needed doing, and following the instructions of the crew. We all worked well as a team, everyone remained very calm and understood our roles, under the excellent leadership of ****.
Having helped transport the patient into the back of the ambulance, and retrieving all of the kit for the paramedic I left the house not knowing what the outcome might be. What I did know, however, was that survival rates for an out of hospital cardiac arrest are less than 1 in 10 – the chances were slim.
I wanted to be sure the neighbour who administered CPR was reassured that she had done everything she could have done for the patient. I didn’t know how I was going to cope with the events of that evening when the adrenelin finally wore off, but I knew I may never see her again to tell her.
Two days after the event, not knowing what the outcome was, I received the following email from EMAS. Unfortunately the outcome wasn’t good, however the feedback reassured me that the training had kicked in, I did everything I possibly could for the family of the patient and was as of much assistance to the Paramedics as I could be.
Hi Alex,
Below are some glowing comments from a paramedic that was very appreciative and impressed by the support you gave him at a cardiac arrest. He appears to be very impressed with the manor of the support and the calm way you went about supporting him.
Thank you for all your support and I will make sure that this is kept on your file.
Kind regards
***
______________________
Hi I just wondered whether you would be able to pass on an official thank-you to the Hinckley CFR ‘Alex’ who was first on scene to a cardiac arrest in ******* yesterday. He was a credit to the CFR team – establishing control of the situation prior to my arrival and providing very high quality assistance (over and above what I would normally expect from a community first responder) throughout the resuscitation attempt. Although ultimately unsuccessful he was instrumental in achieving a ROSC twice and I know for a fact that the family were extremely grateful of the effort that he put in.
Kind Regards
**** ****** – Paramedic, Hinckley Station.
As with any big event in life – good or bad; it’s important to reflect on what happened identify learning opportunities, areas for improvement or maybe an assurance that from someone you respect telling you that you did a good job.
That will be a job, and feedback I’ll never forget.
Two days of responding in a while and I’ve been all over Hinckley – the shifts have been a little up and down, and that’s not just because of the trip to the fairground and to the patient who had fallen from a tree!
As a CFR getting feedback from the amazing guys and gals in green is a really important part of the job. CFRs receive a significant amount of training by EMAS but there is nothing quite like experience, and getting feedback on how you performed. Technicians and Paramedics get lots of experience but the reality of being a CFR is that the likelihood of going to a new type job you’ve not seen before is quite high and this is part of the appeal. It makes the role exciting and unpredictable – just like all of the good things in life.
I always operate within my scope of practice and EMAS guidelines, as every CFR should, but there’s a whole lot of grey between right and wrong. Especially when it comes to something as complex as a human being.
If a Paramedic tells me they would have made a different judgement call, I’m really interested in knowing why. Not “why did you say it like that”. Not “why are you being so critical I’m just a volunteer”.
I’m a big believer in criticism, and I make it constructive even if they don’t. Try this in your walk of life, don’t take things personally and see how you get on.
Step back and look at the situation objectively and understand why you did what you did. If you can’t logically justify your actions to yourself you can’t understand what led you to act in a certain way. Don’t try to justify your actions with the intention of convincing yourself you were right or wrong, do it to really understand why you did what you did. Now you can begin to think about why someone else, in this case the Paramedic, would have done things differently. If you’re struggling, talk to someone else about it. Read up on the subject. You should now be open minded on the subject and better placed to know what you should do next time (this might be exactly the same as you did this time!).
In fact, even if the feedback is positive, like the feedback I received from a Community Paramedic this morning after attending a 5 year old with breathing difficulties. I still review how I performed, and why I did what I did.
Community first responders (CFRs) are in schemes founded and run by volunteers who give up their spare time to attend appropriate emergency calls in their own community. They are dispatched by the EMAS Emergency Operations Centre.
EMAS always provides the fastest possible response to emergency calls using its conventional resources such as ambulances and fast response cars. However, for patients experiencing cardiac arrest every second counts. For every minute that passes without defibrillation a person’s chances of survival can decrease by up to 10%.
In the more rural and hard to reach areas of the East Midlands, community first responders have a much better chance of providing the immediate help needed prior to the arrival of an EMAS crew.
All CFRs are trained to a high level by EMAS over a series of multi-day courses. Regular training sessions are held by the group and annual requalifications in Basic Life Support (BLS) and Drugs are mandatory.